

Patient with congenitally missing lateral incisors. The S.M.A.R.T. minimally invasive bone grafting technique provides predictable horizontal bone augmentation with fewer complications, less pain and swelling. S.M.A.R.T. bone graft was performed on both lateral incisor sites using a single incision.

The S.M.A.R.T. approach facilitates flapless implant placement, which may be followed by delivery of a temporary restoration. This results in fewer procedures compared to traditional techniques. Treatment duration is decreased, with less discomfort and less expense to the patient, while preserving soft tissue architecture.

S.M.A.R.T. bone graft helps to enhance the esthetic appearance of implant restorations. The presence of sufficient bone volume makes ideal implant placement possible, facilitating natural restorative contours and emergence profiles.

The buccal plate of bone can be predictably augmented with the S.M.A.R.T. technique to optimize the site prior to implant placement. This represents a change in the paradigm for immediate implant placement and provisionalization, forcing a re-evaluation concepts regarding gap size and preservation of buccal contours.

TREATMENT OF EXPOSED IMPLANT SURFACES
Bone regeneration over exposed implant surfaces is a novel application of the S.M.A.R.T. technique. Bone may be absent for a variety of reasons, usually related to placement or bone remodeling.

As bone loss advances, implants may need to be removed and treatment started all over again. Traditional techniques have shown limited success in regenerating bone over implants. The S.M.A.R.T. technique has been successful in treating exposed implant surfaces with up to 3 year follow up. It provides a simplified, predictable and cost-effective alternative, with less patient discomfort.

COMPLEX CASE
Knife-edge ridge after failed implant and bone graft. The patient did not want to have a block graft or a hip graft and was referred for S.M.A.R.T. minimally invasive bone grafting.

S.M.A.R.T. bone graft was performed in a 45-minute visit. Adjacent teeth with thin or missing bone were also treated. Graft was performed from canine to canine with a single incision.

Flapless implant placement was performed 6 months later. The implant supported restoration was completed 1-year ago.

COMPLEX CASE
Patient suffered a traumatic injury at age 12. Five implants were placed during his early 20’s that subsequently failed. Implants were removed and repeated bone grafting procedures were unsuccessful, resulting in inadequate bone volume for implants and heavy scar formation. Patient was eventually referred to our office for augmentation of the severely maxillary anterior residual ridge.

S.M.A.R.T. VERTICAL & HORIZONTAL AUGMENTATION
Performed in a single office procedure using local anesthesia and two small incisions. No flaps, no tenting screws and no membranes were utilized. Sufficient horizontal and vertical bone volume was achieved to allow future placement of multiple implants.

Substantial vertical augmentation in the area of the failed anterior implants accomplished with the S.M.A.R.T. method. The patient reported minimal pain and moderate swelling. Periosteal elevation was difficult due to extensive scar tissue.

Implants were placed 9 months following the S.M.A.R.T. bone graft. Bone in the vertically grafted areas was hard to drill through the osteotomy process. All implants exhibited excellent primary stability.

With the patient’s consent, a core specimen was harvested during the osteotomy preparation for implant #9(21) and sent for histologic analysis.
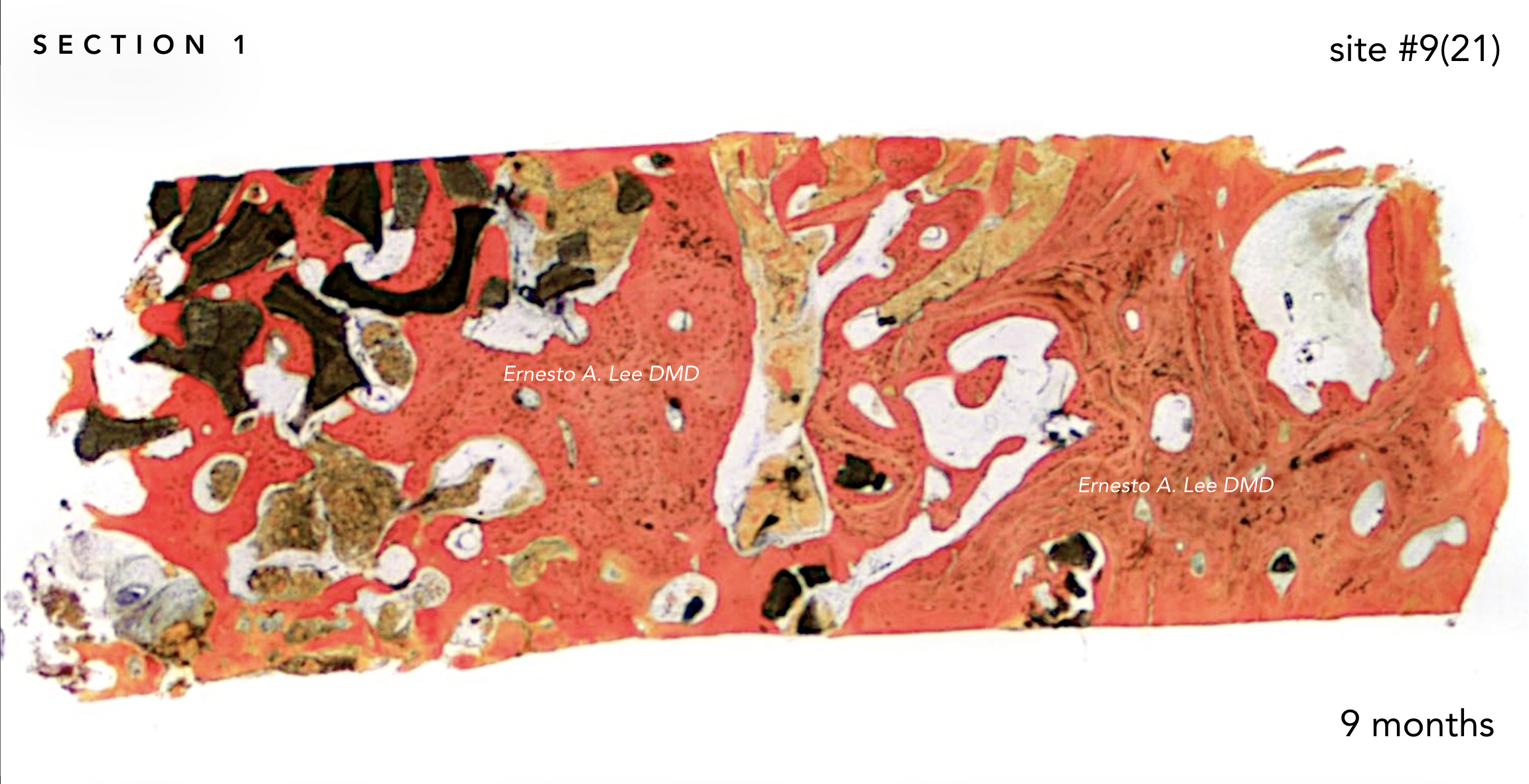







The interstitial and concentric lamellar bone patterns observed are consistent with the appearance of healthy, orderly, living bone.


With the patient's authorization, a specimen was harvested during the osteotomy preparation for implant on site #9(21) and sent for histologic analysis.

Vertical and horizontal augmentation of thin mandibular posterior ridge. The patient sought a minimally invasive approach, having previously declined treatment proposals that included hip and block grafts.

S.M.A.R.T. Vertical and horizontal mandibular ridge augmentation. Once again, no flaps, tenting screws or membranes were used. Compared to traditional GBR/block/hip grafting techniques...this was a 45 minute in-office procedure, with less pain, less swelling and fewer potential complications. Implants will be placed following a 6-month healing period.
